An aHUS diagnosis, lucky or what?
It is hard to believe that it will soon be two years since the aHUS Diagnosis Process project began. It began…
It is hard to believe that it will soon be two years since the aHUS Diagnosis Process project began. It began…
The most important conference being held this year to feature aHUS, is the long awaited ISN Complement Mediated Renal Disease meeting…
65 questions, 29 article blogs with answers to the questions published between 7 March and 16 May and over 300 views…
A final question in the RDD2022 video series on how to integrate a patient voice of experience into aHUS Pharma and…

This question about difference in disease triggers and treatments from Jeff did not feature in the RDD2022 video but was given…
A number of questions in the RDD2022 video are about what will happen to patients in the future due to the…
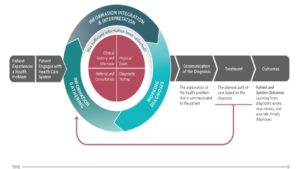
The care pathway for aHUS patients has been looked at in detail in Global Action’s Diagnosis Process Study ( for reports…
Zinovieva asked two related questions in the RDD 2020 video The issues of what provokes ( or triggers) the development of…
Ravulizumab is more widely used these days, particularly in the PNH community. Apart from the longer infusion intervals PNH patients benefit…