
News from Japan
One of the newest alliance affiliates is aHUS Kids Japan although it hard to believe that it was formed over two…
One of the newest alliance affiliates is aHUS Kids Japan although it hard to believe that it was formed over two…

A meeting of the aHUS alliance is always an opportunity to learn and share news with the aHUS patient community globally.…

Atypical HUS in the Netherlands - An aHUS Alliance interview with the Dutch research and clinical teams at Radboudumc, to include the broad importance of their CUREiHUS study and its potential impact for patients and physicians world wide.
Another webinar by ERKNet of interest to the aHUS community was held today. It was to be given by Dr Giuseppe…

In April 2013 we heard that NICE would not get to the evaluating and decision step until December 2013 , which…

The Dutch aHUS patients' conference is being held in Nimegen and the participants are gathering at the Fletcher Park Hotel Val…

For the Reluctant Advocate story so far click here NICE was not ready to begin its work on eculizumab when it…
THe Reluctant Advocate series continues.
It continues with the evaluation of eculizumab for aHUS now needing to be carried out by NICE, even though it had already been evaluated and recommended by another group. This was called for by the Health Minister because he wanted a view on whether eculizumab was affordable by the NHS for the treatment of a small number of rare disease patients.
Eculizumab had already been deemed an approved highly specialised technology for the treatment for patients affected by Paroxysmal Nocturnal Haemoglobinuria ,or PNH; so the question now really was “was it affordable for aHUS too?”. What had happened for PNH patients was irrelevant. Neither could support to our cause from those PNH patients be expected.
However it could be said that what was going to happen to us was going to have a bearing on those rare disease patients who were going to follow us in the NICE process. There was a great responsibility on our shoulders.
Affordability. Eculizumab came at a price and NHS England had resources from taxation etc. of over £100 billion , £2 billion a week and rising some might put it. The cost for a small number of rare disease patients was well within its means. So that could not be the test of what affordable means.
The finances and economics of health are both complex and confusing subjects, with inconsistencies throughout, so to get a simple answer for the Health Minister was not going to be straight forward. That was aHUSUK’s worry. An unanswerable question being posed for debate when patients were suffering.
It is at this point that awareness grows that there is no human right to life when it comes to decision processes about providing treatment to patients. This does not mean that those making the decisions do not care about people , it just means that they are protected from any action against their decision on the grounds of abusing human rights to life, because it is ruled not an abuse. Not many people know that.
Another issue which emerges is the lack of clear thinking on financial and economic terms used . In the time aHUSUK had been involved , and particularly in communications supporting the Minister’s decision , we had heard about need for cost effectiveness, reasonable price, wise use of NHS resources , a cash strapped NHS , value for money, value based pricing. All of which mean different things and are mostly subjective in nature with rarely an acceptable established methodology to arrive at an indisputable conclusion.
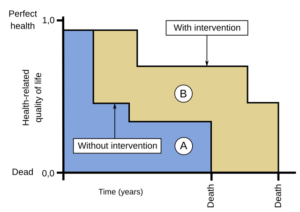
Cost effectiveness in health economics “science” means lower incremental cost per QALY . QALY has been mentioned before and is a difficult concept to understand. Those defending using cost per QALY as a methodology were apt to defend it from critics by saying “ that if you cannot find three flaws in the QALY process you do not understand it “ .
Hardly a ringing endorsement but the flaws apply equally to all and it is the comparative result between treatments which is important.
But cost effectiveness as determined by QALY assessment, although egaliterean , does not necessarily mean affordable. Neither would it be equitable, it would only apply to a small fraction of total NHS spend and would be institutionally discriminatory against those needing ultra orphan drugs. In QALY assessments for aHUS patients their quality of life after treatment would need to be 1 on scale of 0 to 1, having been 0.1; or with eculizumab they would have to live in such perfect health for 300 years or more. Not going to happen.
aHUSUK would focus on affordability being what the “cost”of treating the aHUS patient cohort would be . That would be determined by the number of aHUS patients there were and what the average cost of eculizumab doses needed would be. Quantity x Doses Price. The drug budget.
Following that our focus was on the cost of other uses of NHS resources using the principle that “when escaping from a lion you do not have to run faster than the lion, but just need to run faster than others running away” . That is how NICE would be looking at it effectively , in a cash strapped NHS are there other treatments that are less beneficial that could be given up to afford the treatment of aHUS patients? The opportunity cost as the experts call it I.e. the cost of the foregone alternative.
Thirdly aHUSUK would look deeper into the price of eculizumab and what elements make up its price because for all the academic nature of such health evaluations , the main concern remained “was Alexion’s price for eculizumab a “rip off” of ultimately the tax payers who fund the NHS?”. Making profit was acceptable for the sustained availability of eculizumab, but as the market sales grew and costs of sales reduced and overhead costs fixed , where was that sales growth dividend going?
aHUSUK had come along way since it was formed with barely anything but a personal knowledge of a family member’s encounter with aHUS. The trustees were now learning about concepts and methodologies used by experts , but without the training and experience of these experts. Armed with common sense and a growing confidence in what to challenge and how to do so, we still needed to punch way above our weight, but do it now in a high profile formal evaluation process which was being developed in front of our eyes.
Affordable clearly means a lot more than simply an ability to afford.
Break down in communication flows and fragmented outreach have built barriers for research and clinical trial enrollment regarding advancing new options for those with the rare disease atypical HUS (aHUS, or hemolytic uremic syndrome). The aHUS Alliance looks at current challenges, and potential pathways to explore and engage.