Remission from aHUS is different from having been cured because there is still an uncertainty that aHUS can return. If that happens it is called a relapse. For a relapse to happen something needs to trigger another episode of uncontrolled Complement, because the patient will still have a predisposing genetic mutation in one or more of their Complement System components. Or something returns , like anti factor h autoantibodies , to hamper the control of their Complement.
It is difficult to say with any certainty how long someone will stay in remission, Jaxson. Nor indeed to say whether definitely some will never relapse , Yoann and remain in remission for life.
It is better to think of it terms of likelihood of remission and a risk of relapse Jaxson.
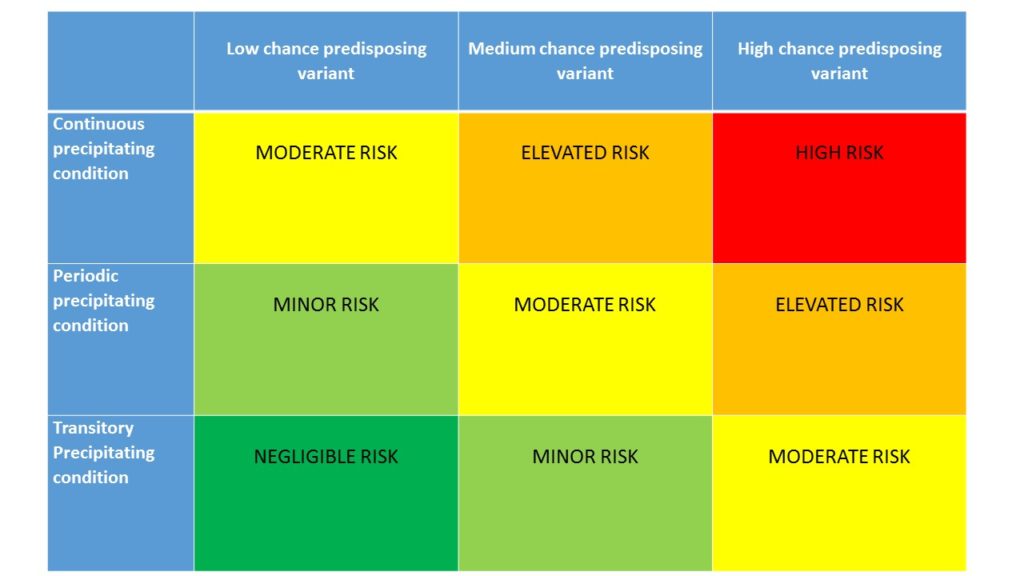
In the table that Global Action created to illustrate this (see below) , the outcome is graded from high risk of relapse (red) or unlikely continuous remission to negligible risk of relapse (green) or likely continuous remission. And there are three levels of risk, elevated , moderate or minor, or likely remission, in between the red and green rectangles. in descending order, or ascending, depending on whether it is relapse or remission is being looked at.
Each is dependent on the type of precipitating genetic mutation that the patient has , or does not havs ( idiopathic ) and the strength and continuity of triggers encountered. Some triggers maybe periodic, like infections , or transitory, like pregnancy, but others like a kidney transplant would be continuous.
Someone with a CFH mutation and kidney graft would probably be placed in the red box. Someone with no mutation and having given birth may be placed in the dark green box. And so on. But most would likely fall between the extremes in elevated, moderate or minor risk/likelihood of relapse or remission.
The chance of relapse diminishes with time Lisa. If it is going to happen, it often does in the first six months. After that it can still happen based on the factors illustrated in the Global Action matrix. It takes time to be more confident about it but self monitoring can help with any initial anxiety. Your remission may last for life or long enough to have several relapses with a gap of years in between. With short term eculizumab treatment in between. ( Update : Lisa has told us that since she asked the question for the video, and after withdrawal from treatment for only three months, she has relapsed with aHUS and is back on treatment.)
Could it be a way of life as Paige asks?. Something that interrupts from time to time but which can be managed so that it is small part of who people are. Knowing that a swift return to treatment avoids any further damage. Not in denial but accepting a new normal. A personal choice.

Having a relapse may be a predictor of further relapses, Joris. But although your genetics may remain the same , the triggering “environment” may change. It takes many hits for aHUS to breakthrough.
Perhaps in time doctors will categorise all triggers into continuous , periodic or transitional and all the different genetic mutations into low , medium , or high risk and create a predictive tool for all patients asking these questions.
When will that be is another question?!
But when ever it does, hopefully it will be based on what happens to every patient around the world and their specific experiences of relapse and remission, and will help other aHUS patients in the future.

{kind=link}