aHUS Patients contributed two questions to the aHUS Patients Research Agenda:
1. Is there an optimal way in which a complement inhibitor can be delivered to suit an individual’s need ?
2. Can a complement inhibitor be stopped safely when not needed by some aHUS patients and what makes them different?
Dr Gema Ariceta a leading aHUS researcher and paediatrician from Spain recently had an article published ( full article can be seen here) which looks for scientific evidence.
The title of her article is “Optimal dosing of eculizumab for atypical Haemolytic Uraemic Syndrome (aHUS) – a question to be addressed in a scientific way
Gema’s paper ,after the usual introductions to aHUS and the Complement inhibitor eculizumab focuses on the many published results about studies done so far , including those from Radboud University Nijmegen and the aHUS Expert Centre in Milan which have featured in news blogs on the alliance website.
This type of research is known as a “literature review” and is very important to establish a position at a point in time about what is known and what is not known about a particular topic . The unknowns are for the future.
Gema’s article provides an interim answer from the literature to the aHUS Patients questions.
1. Yes some evidence but not universally applicable
2A Yes for some
2B Those without an identified Complement mutation and those whose aHUS is the result of antifactor H Antibodies are strong candidates
However Gema makes the valid observation that what is needed is a rigorous prospective international collaborative approach to provide proof and guidelines for aHUS management. It needs to be science driven and practical.
It may also all have to be redone if and when ravulizumab, the longer lasting eculizumab, is marketed. For ravulizumab , the highest dose ( Over 100kg Patient) at eight week intervals will be 12 vials only three quarters of the 16 vials of eculizumab over the same period. Other weight patients will get less but no information yet on patients weight up to 40kg.
Some aHUS patients with tapering strategies at present currently only receive six vials of ecu in that same period. Alexion has said that Ravu will come with a 10% discount.
The alliance supports Gema’s view. One size fits all may not be right neither economically nor clinically needed , but neither is blind action on a “suck it and see basis” a safe way , nor the helpful way for others, to go about it.
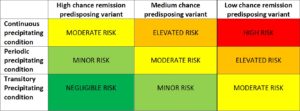
The likelihood of continuing TMA control , or TMA return, depends on predisposition factors and precipitating conditions . aHUS Patients come at varying risks to these , from high risk to negligible ( no one says no risk) for both.
Would it be helpful for aHUS patients to know where they would be placed in a risk matrix like the one below and understand what treatment decisions based on it are best for them.?
Those with no detectable complement mutation ,or AFHAs might be in the lime greeen boxes but those with CFH mutations in the red or at the top edges of the orange boxes.
Can science give the answers?

{kind=link}